


 Sign Out
Sign Out



Pharmacodynamic effects: Paliperidone is a centrally active dopamine Type 2 (D2) receptor antagonist and a serotonin Type 2 (5HT2A) receptor antagonist. Paliperidone is also active as an antagonist at α1 and α2 adrenergic receptors and H1 histaminergic receptors, which may explain some of the other effects of the drug. Paliperidone has no affinity for cholinergic muscarinic or β1- and β2-adrenergic receptors. The pharmacological activity of the (+)- and (-)- paliperidone enantiomers is qualitatively and quantitatively similar in vitro.
Clinical Studies: Schizophrenia: Short-Term Monotherapy (Studies 1, 2, 3, 4): The efficacy of INVEGA SUSTENNA in the acute treatment of schizophrenia was evaluated in four short-term (one 9-week and three 13-week) double-blind, randomized, placebo-controlled, fixed-dose studies of acutely relapsed adult inpatients who met DSM-IV criteria for schizophrenia. The fixed doses of INVEGA SUSTENNA in these studies were given on days 1, 8, and 36 in the 9-week study, and additionally on day 64 of the 13-week studies, i.e., at a weekly interval for the initial two doses and then every 4 weeks for maintenance.
Efficacy was evaluated using the total score on the Positive and Negative Syndrome Scale (PANSS). The PANSS is a 30 item scale that measures positive symptoms of schizophrenia (7 items), negative symptoms of schizophrenia (7 items), and general psychopathology (16 items), each rated on a scale of 1 (absent) to 7 (extreme); total PANSS scores range from 30 to 210.
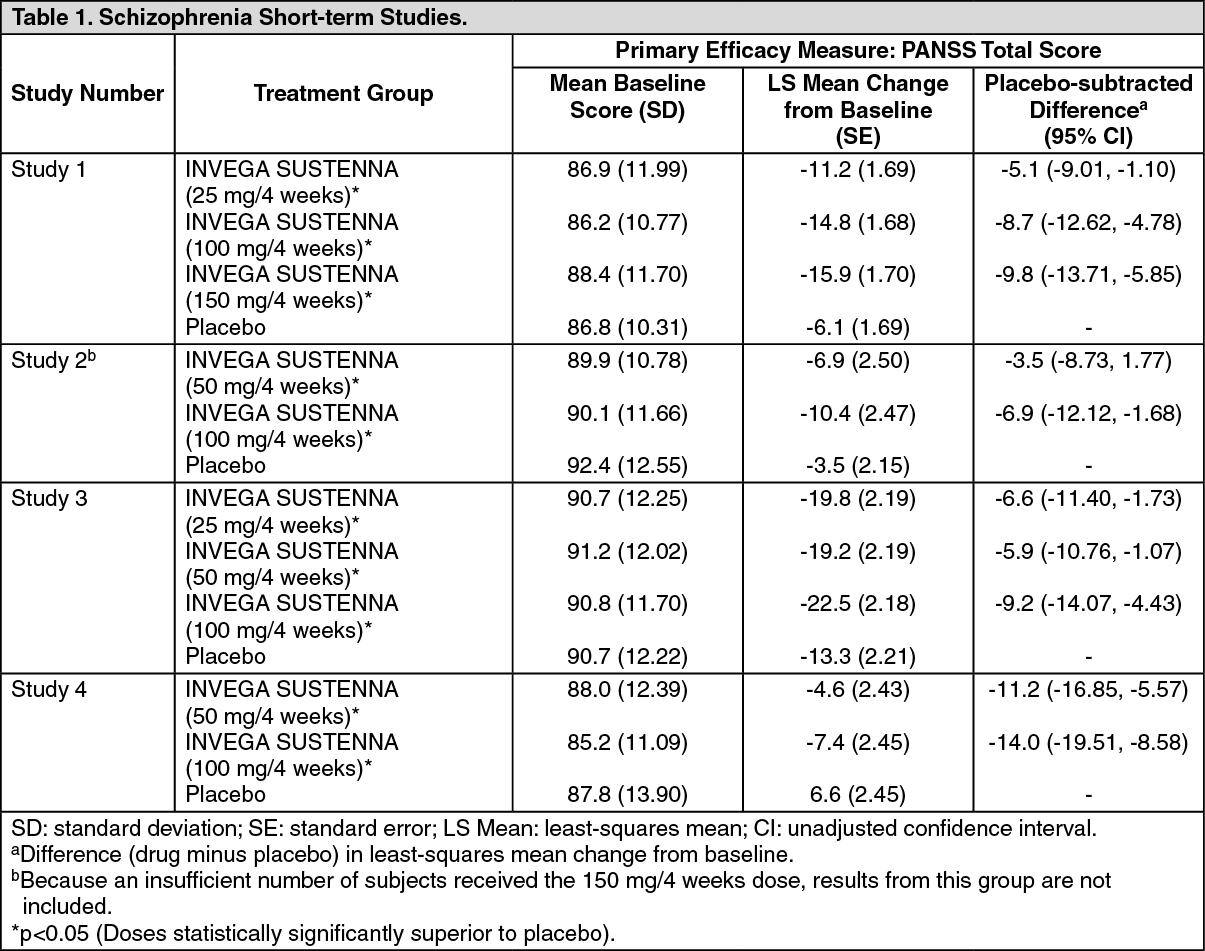
In Study 1 (PSY-3007), a 13-week study (n=636) comparing three fixed doses of INVEGA SUSTENNA (initial deltoid injection of 150 mg followed by 3 gluteal or deltoid doses of either 25 mg/4 weeks, 100 mg/4 weeks or 150 mg/4 weeks) to placebo, all three doses of INVEGA SUSTENNA were superior to placebo in improving the PANSS total score.
In Study 2 (PSY-3003), another 13-week study (n=349) comparing three fixed doses of INVEGA SUSTENNA (50 mg/4 weeks, 100 mg/4 weeks, and 150 mg/4 weeks) to placebo, only 100 mg/4 weeks of INVEGA SUSTENNA was superior to placebo in improving the PANSS total score.
In Study 3 (PSY-3004), a third 13-week study (n=513) comparing three fixed doses of INVEGA SUSTENNA (25 mg/4 weeks, 50 mg/4 weeks, and 100 mg/4 weeks) to placebo, all three doses of INVEGA SUSTENNA were superior to placebo in improving the PANSS total score.
In Study 4 (SCH-201), the 9-week study (n=197) comparing two fixed doses of INVEGA SUSTENNA (50 mg/4 weeks and 100 mg/4 weeks) to placebo, both doses of INVEGA SUSTENNA were superior to placebo in improving PANSS total score.
A summary of the mean baseline PANSS scores along with the mean changes from baseline in the four short-term acute schizophrenia studies are provided in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
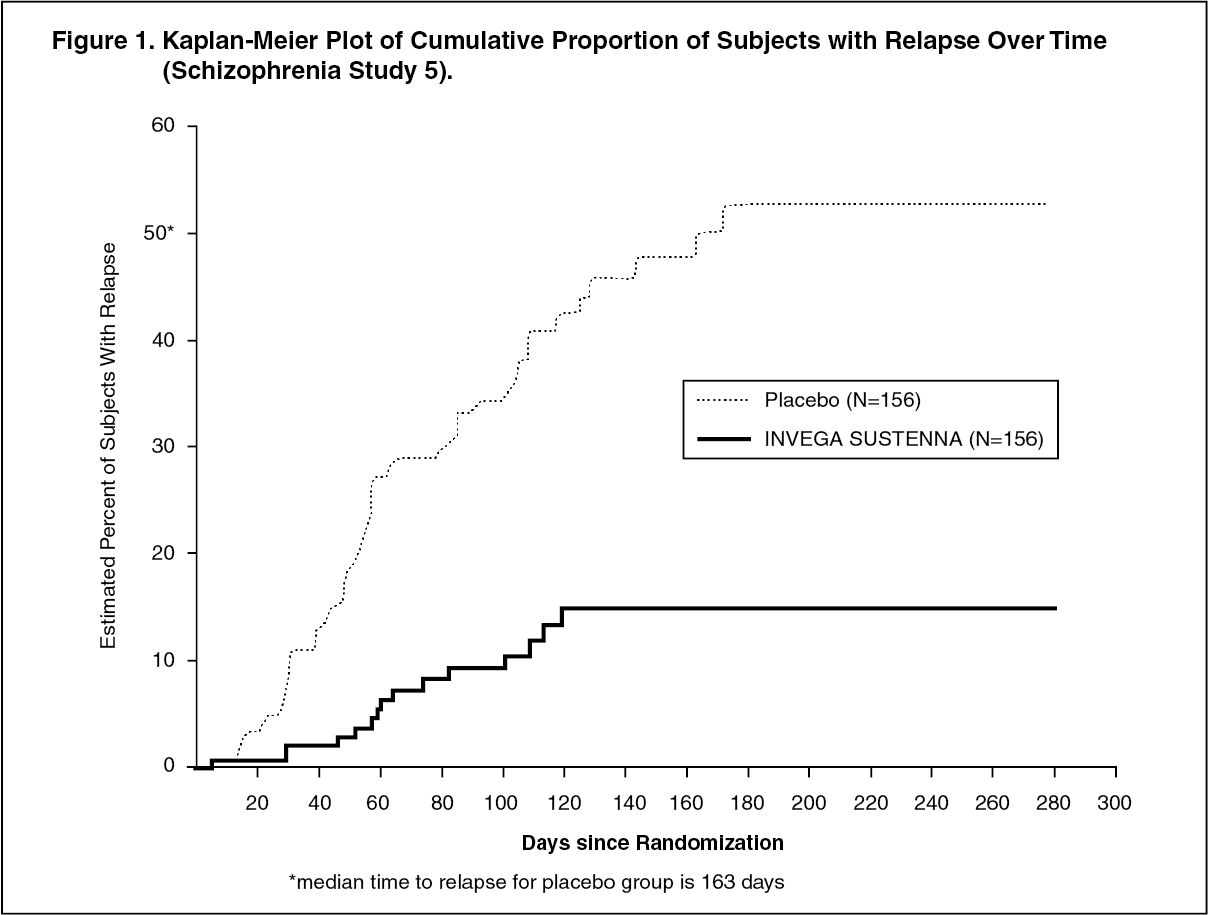
Click on icon to see table/diagram/imageMaintenance Monotherapy Treatment (Study 5: PSY-3001): The efficacy of INVEGA SUSTENNA in maintaining symptomatic control in schizophrenia was established in a longer-term double-blind, placebo-controlled, flexible-dose study involving adult subjects who met DSM-IV criteria for schizophrenia. This study included a minimum 12-week, fixed-dose stabilization phase, and a randomized, placebo-controlled phase to observe for relapse. During the double-blind phase, patients were randomized to either the same dose of INVEGA SUSTENNA they received during the stabilization phase, i.e., 25 mg, 50 mg, or 100 mg administered every 4 weeks, or to placebo. A total of 410 stabilized patients were randomized to either INVEGA SUSTENNA or to placebo until they experienced a relapse of schizophrenia symptoms. Relapse was pre-defined as time to first emergence of one or more of the following: psychiatric hospitalization, ≥ 25% increase (if the baseline score was > 40) or a 10-point increase (if the baseline score was ≤ 40) in total PANSS score on two consecutive assessments, deliberate self-injury, violent behavior, suicidal/homicidal ideation, or a score of ≥ 5 (if the maximum baseline score was ≤ 3) or ≥ 6 (if the maximum baseline score was 4) on two consecutive assessments of the specific PANSS items. The primary efficacy variable was time to relapse. A pre-planned interim analysis showed a statistically significantly longer time to relapse in patients treated with INVEGA SUSTENNA compared to placebo, and the study was stopped early because maintenance of efficacy was demonstrated. Thirty-four percent (34%) of subjects in the placebo group and 10% of subjects in the INVEGA SUSTENNA group experienced a relapse event. There was a statistically significant difference between the treatment groups in favor of INVEGA SUSTENNA. A Kaplan-Meier plot of time to relapse by treatment group is shown in Figure 1. The time to relapse for subjects in the placebo group was statistically significantly shorter than for the INVEGA SUSTENNA group. An examination of population subgroups did not reveal any clinically significant differences in responsiveness on the basis of gender, age, or race. (See Figure 1.)
 Click on icon to see table/diagram/image
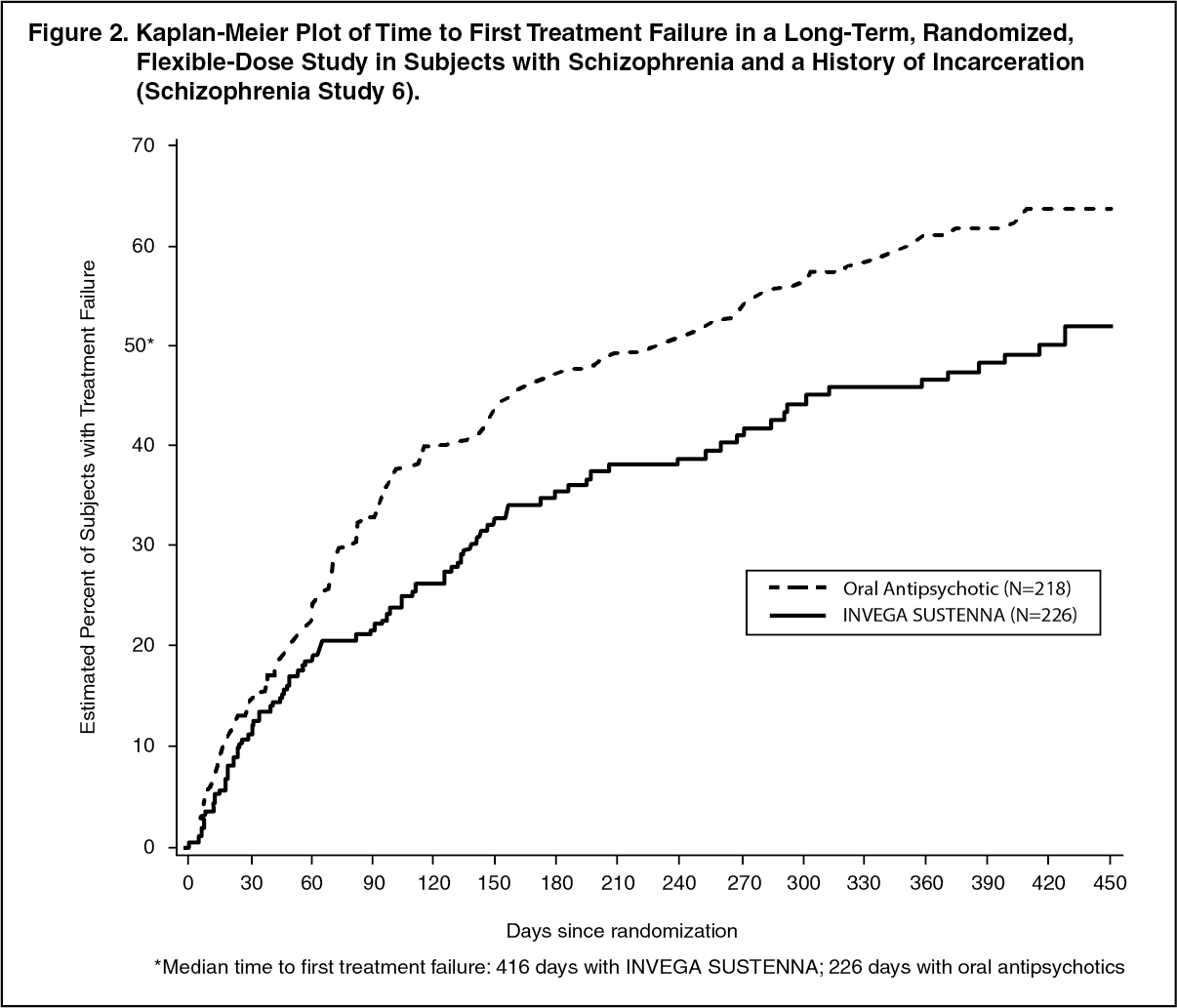
Click on icon to see table/diagram/imageLong-Term Comparative Monotherapy Treatment versus Oral Antipsychotic Therapy (Study 6: SCH-3006): The efficacy of INVEGA SUSTENNA in delaying time to treatment failure compared with selected oral antipsychotic medications was established in a long-term, randomized, flexible-dose study in subjects with schizophrenia and a history of incarceration. Subjects were screened for up to 14 days followed by a 15-month treatment phase during which they were observed for treatment failure.
The primary endpoint was time to first treatment failure. Treatment failure was defined as one of the following: arrest and/or incarceration; psychiatric hospitalization; discontinuation of antipsychotic treatment because of safety or tolerability; treatment supplementation with another antipsychotic because of inadequate efficacy; need for increase in level of psychiatric services to prevent an imminent psychiatric hospitalization; discontinuation of antipsychotic treatment because of inadequate efficacy; or suicide. Treatment failure was determined by an Event Monitoring Board (EMB) that was blinded to treatment assignment. A total of 444 subjects were randomly assigned to either INVEGA SUSTENNA (N = 226; median dose 100 mg) or one of up to seven pre-specified, flexibly-dosed, commonly prescribed oral antipsychotic medications (N = 218; aripiprazole, haloperidol, olanzapine, paliperidone, perphenazine, quetiapine, or risperidone). The selection of the oral antipsychotic medication was determined to be appropriate for the patient by the investigator. A statistically significantly longer time to first treatment failure was seen for INVEGA SUSTENNA compared with oral antipsychotic medications. The median time to treatment failure was 416 days and 226 days for INVEGA SUSTENNA and antipsychotic medications, respectively. A Kaplan-Meier plot of time to first treatment failure is shown in Figure 2. The frequencies of first treatment failure events by type are shown in Table 2. The time to first arrest and/or incarceration or psychiatric hospitalization was also statistically significantly longer for the INVEGA SUSTENNA group compared to the oral antipsychotic group. (See Figure 2 and Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image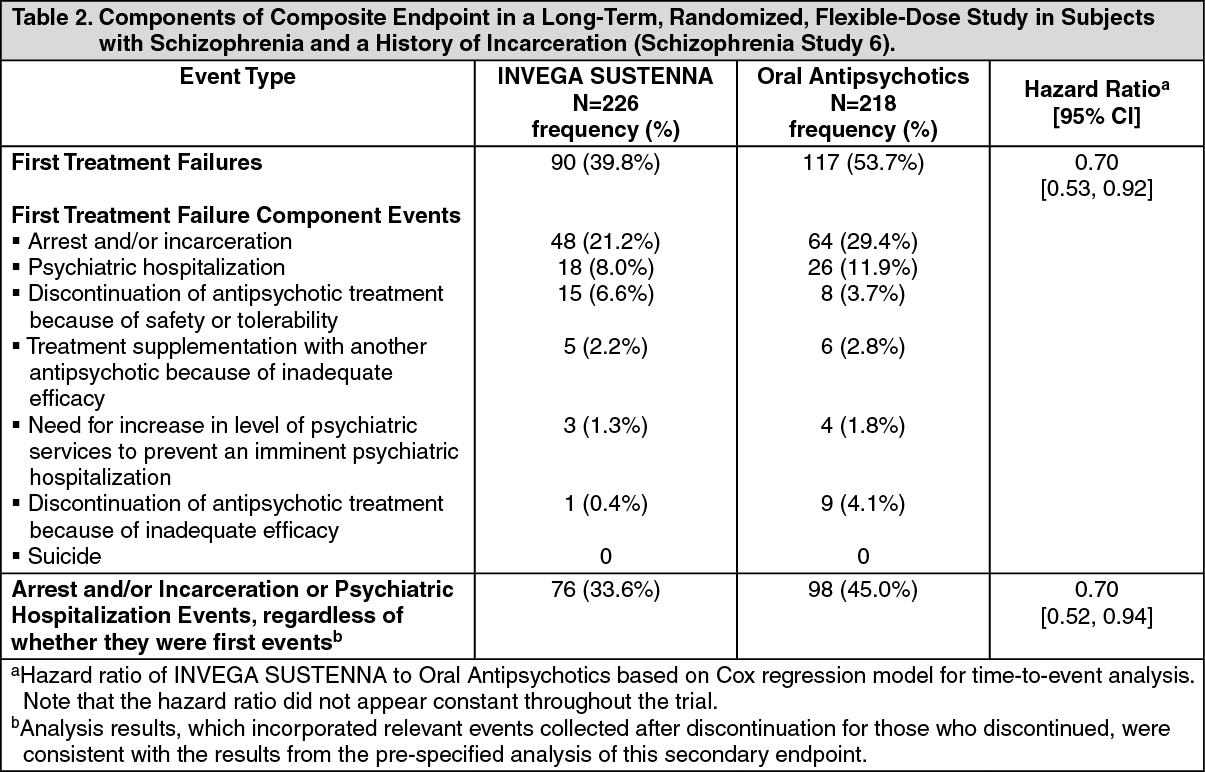 Click on icon to see table/diagram/image
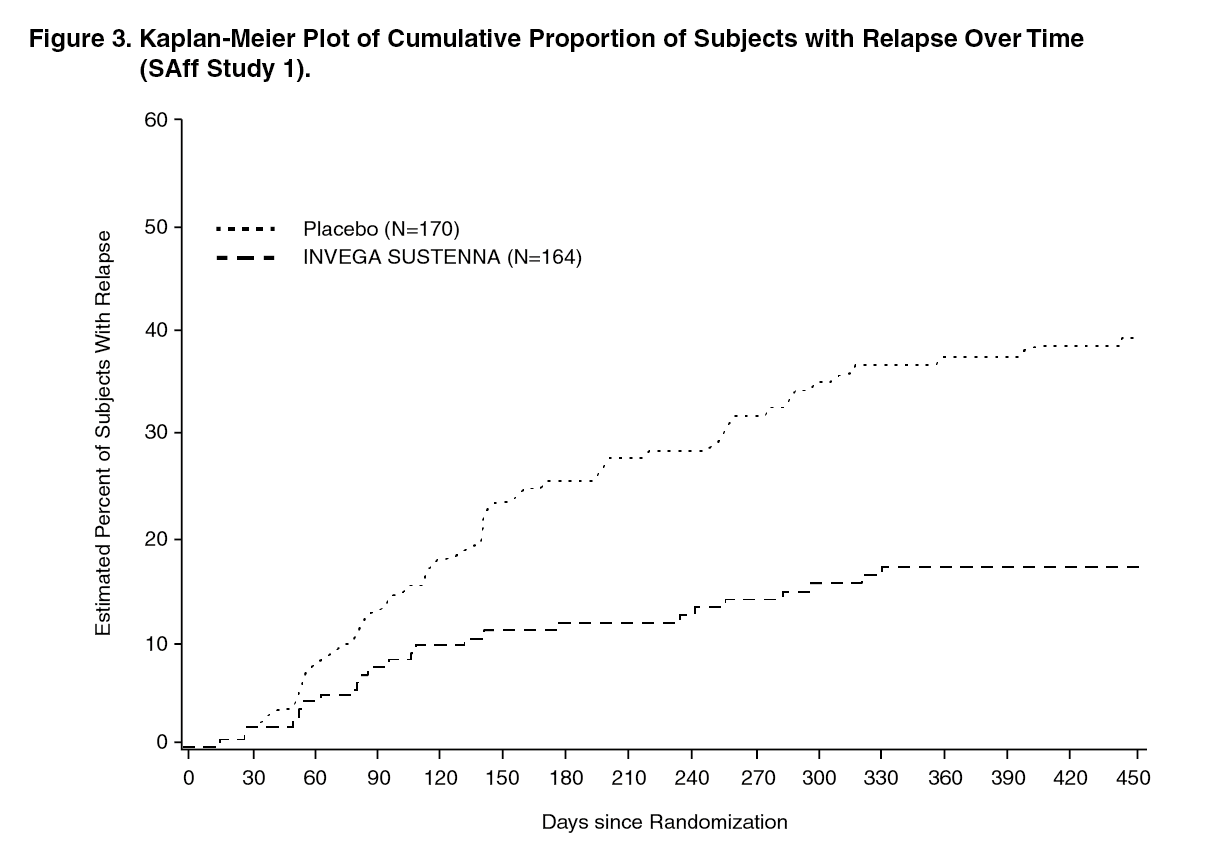
Click on icon to see table/diagram/imageSchizoaffective Disorder: Maintenance Treatment - Monotherapy and as Adjunct to Mood Stabilizer or Antidepressant (SAff Study 1: SCA-3004): The efficacy of INVEGA SUSTENNA in maintaining symptom control in schizoaffective disorder was established in a long-term double-blind, placebo-controlled, flexible-dose randomized-withdrawal study designed to delay relapse in adult subjects who met DSM-IV criteria for schizoaffective disorder, as confirmed by the Structured Clinical Interview for DSM-IV Disorders. The population included subjects with schizoaffective bipolar and depressive types. Subjects received INVEGA SUSTENNA either as monotherapy or as an adjunct to stable doses of antidepressant or mood stabilizers.
This study included a 13-week, open-label, flexible-dose (INVEGA SUSTENNA 50 mg, 75 mg, 100 mg, or 150 mg) lead-in period which enrolled a total of 667 subjects who had 1) acute exacerbation of psychotic symptoms; 2) score ≥4 on ≥3 PANSS items of delusions, conceptual disorganization, hallucinatory behavior, excitement, suspiciousness/persecution, hostility, uncooperativeness, tension, and poor impulse control; and 3) prominent mood symptoms ≥16 on the Young Mania Rating Scale (YMRS) and/or the Hamilton Rating Scale for Depression, 21-item version (HAM-D-21). Subjects were 19 to 66 years old (mean 39.5 years) and 53.5% were male. The mean scores at open-label enrollment of PANSS total was 85.8 (range 42 to 128), HAM-D-21 was 20.4 (range 3 to 43), YMRS was 18.6 (range 0 to 50), and CGI-S-SCA was 4.4 (range 2 to 6).
After the 13-week open-label flexible-dose INVEGA SUSTENNA treatment, 432 subjects met stabilization criteria (PANSS total score ≤70, YMRS ≤12, and HAM-D-21 ≤12) and continued into the 12-week open-label fixed-dose stabilization period.
A total of 334 subjects who met stabilization criteria for 12 consecutive weeks were randomized (1:1) to continue the same dose of INVEGA SUSTENNA or to placebo in the 15-month, double-blind, maintenance period. For the 164 subjects who were randomized to INVEGA SUSTENNA, dose distribution was 50 mg (4.9%), 75 mg (9.8%), 100 mg (47.0%), and 150mg (38.4%). The primary efficacy variable was time to relapse. Relapse was defined as the first occurrence of one or more of the following: 1) psychiatric hospitalization; 2) intervention employed to avert hospitalization; 3) clinically significant self-injury, suicidal or homicidal ideation or violent behavior; 4) a score of ≥6 (if the score was ≤4 at randomization) of any of the individual PANSS items: delusions, conceptual disorganization, hallucinatory behavior, excitement, suspiciousness/persecution, hostility, uncooperativeness, or poor impulse control; 5) on two consecutive assessments within 7 days: ≥25% increase (if the score at randomization was >45) or ≥10-point increase (if the score at randomization was ≤45) in total PANSS score; a score of ≥5 (if the score was ≤3 at randomization) of any of the individual PANSS items: delusions, conceptual disorganization, hallucinatory behavior, excitement, suspiciousness/persecution, hostility, uncooperativeness, or poor impulse control; an increase of ≥2 points (if the score was 1 [not ill] to 3 [mildly ill] at randomization) or increase of ≥1 point (if the score was ≥4 [moderately ill or worse] at randomization) in CGI-S-SCA overall score.
There was a statistically significant difference in time to relapse between the treatment groups in favor of INVEGA SUSTENNA. A Kaplan-Meier plot of time to relapse by treatment group is shown in Figure 3. (See Figure 3.)
 Click on icon to see table/diagram/image
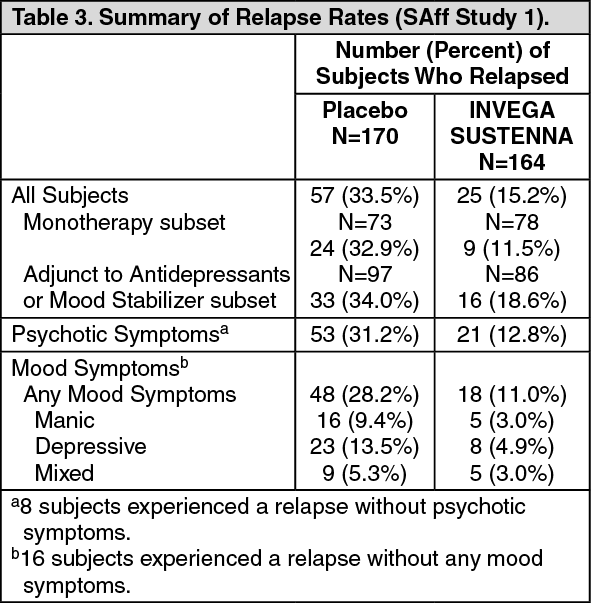
Click on icon to see table/diagram/imageTable 3 summarizes the number of subjects with relapse in the overall population, by subgroup (monotherapy vs. adjunctive therapy), and by symptom type at the first occurrence of relapse. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePharmacokinetics: Absorption and Distribution: Due to its extremely low water solubility, the 1-month formulation of paliperidone palmitate dissolves slowly after intramuscular injection before being hydrolyzed to paliperidone and absorbed into the systemic circulation. Following a single intramuscular dose, the plasma concentrations of paliperidone gradually rise to reach maximum plasma concentrations at a median Tmax of 13 days. The release of the drug starts as early as day 1 and lasts for as long as 126 days.
Following intramuscular injection of single doses (25 mg - 150 mg) in the deltoid muscle, on average, a 28% higher Cmax was observed compared with injection in the gluteal muscle. The two initial deltoid intramuscular injections of 150 mg on day 1 and 100 mg on day 8 help attain therapeutic concentrations rapidly. The release profile and dosing regimen of INVEGA SUSTENNA results in sustained therapeutic concentrations. The AUC of paliperidone following INVEGA SUSTENNA administration was dose-proportional over a 25 mg - 150 mg dose range, and less than dose-proportional for Cmax for doses exceeding 50 mg. The mean steady-state peak:trough ratio for an INVEGA SUSTENNA dose of 100 mg was 1.8 following gluteal administration and 2.2 following deltoid administration.
Following administration of paliperidone palmitate the (+) and (-) enantiomers of paliperidone interconvert, reaching an AUC (+) to (-) ratio of approximately 1.6-1.8.
Based on a population analysis, the apparent volume of distribution of paliperidone is 391 L. The plasma protein binding of racemic paliperidone is 74%.
Metabolism and Elimination: In a study with oral immediate-release 14C-paliperidone, one week following administration of a single oral dose of 1 mg immediate-release 14C-paliperidone, 59% of the dose was excreted unchanged into urine, indicating that paliperidone is not extensively metabolized in the liver. Approximately 80% of the administered radioactivity was recovered in urine and 11% in the feces. Four metabolic pathways have been identified in vivo, none of which accounted for more than 10% of the dose: dealkylation, hydroxylation, dehydrogenation, and benzisoxazole scission. Although in vitro studies suggested a role for CYP2D6 and CYP3A4 in the metabolism of paliperidone, there is no evidence in vivo that these isozymes play a significant role in the metabolism of paliperidone. Population pharmacokinetics analyses indicated no discernible difference on the apparent clearance of paliperidone after administration of oral paliperidone between extensive metabolizers and poor metabolizers of CYP2D6 substrates.
The median apparent half-life of paliperidone following INVEGA SUSTENNA single-dose administration over the dose range of 25 mg - 150 mg ranged from 25 days - 49 days.
Long-Acting Paliperidone Palmitate Injection versus Oral Extended-Release Paliperidone: INVEGA SUSTENNA is designed to deliver paliperidone over a monthly period while extended-release oral paliperidone is administered on a daily basis. The initiation regimen for INVEGA SUSTENNA (150 mg/100 mg in the deltoid muscle on Day 1/Day 8) was designed to rapidly attain steady-state paliperidone concentrations when initiating therapy without the use of oral supplementation.
In general, overall initiation plasma levels with INVEGA SUSTENNA were within the exposure range observed with 6-12 mg extended-release oral paliperidone. The use of the INVEGA SUSTENNA initiation regimen allowed patients to stay in this exposure window of 6-12 mg extended-release oral paliperidone even on trough pre-dose days (Day 8 and Day 36). The intersubject variability for paliperidone pharmacokinetics following delivery from INVEGA SUSTENNA was lower relative to the variability determined from extended-release oral paliperidone tablets. Because of the difference in median pharmacokinetic profiles between the two products, caution should be exercised when making a direct comparison of their pharmacokinetic properties.
Drug Interaction Studies: No specific drug interaction studies have been performed with INVEGA SUSTENNA. The information as follows is obtained from studies with oral paliperidone.
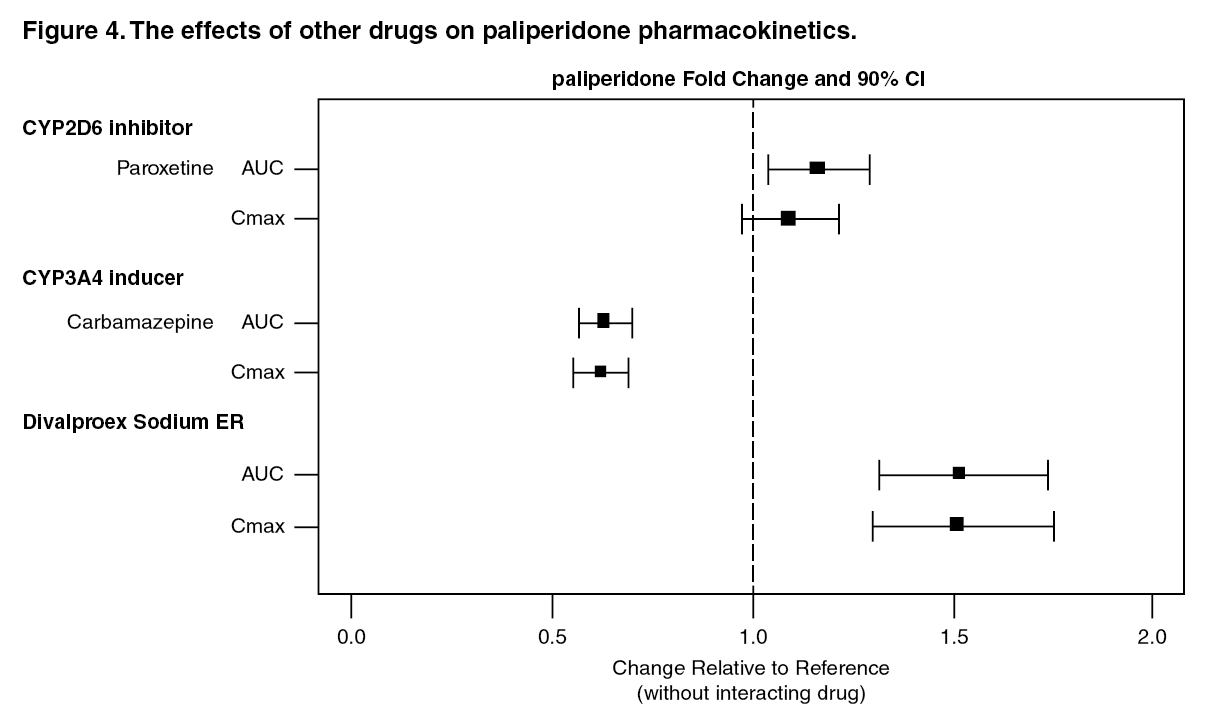
Effects of other drugs on the exposures of paliperidone are summarized in Figure 4. After oral administration of 20 mg/day of paroxetine (a potent CYP2D6 inhibitor), an increase in mean Cmax and AUC values at steady-state was observed (see Figure 4). Higher doses of paroxetine have not been studied. The clinical relevance is unknown. After oral administration, a decrease in mean Cmax and AUC values at steady state is expected when patients are treated with carbamazepine, a strong inducer of both CYP3A4 and P-gp (see Drugs Having Clinically Important Interactions with INVEGA SUSTENNA under Interactions). This decrease is caused, to a substantial degree, by a 35% increase in renal clearance of paliperidone. (See Figure 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageClinically meaningful pharmacokinetic interaction between INVEGA SUSTENNA and valproate (including valproic acid and divalproex sodium) is not expected. Oral administration of divalproex sodium extended-release tablets (two 500 mg tablets once daily at steady-state) with oral paliperidone extended-release tablets resulted in an increase of approximately 50% in the Cmax and AUC of paliperidone.
After oral administration of paliperidone, the steady-state Cmax and AUC of divalproex sodium extended-release tablets were not affected in 13 patients stabilized on divalproex sodium extended-release tablets. In a clinical study, subjects on stable doses of divalproex sodium extended-release tablets had comparable valproate average plasma concentrations when oral paliperidone extended-release tablets 3-15 mg/day was added to their existing divalproex sodium extended-release tablets treatment (see Drugs Having No Clinically Important Interactions with INVEGA SUSTENNA under Interactions).
In vitro studies indicate that CYP2D6 and CYP3A4 may be involved in paliperidone metabolism, however, there is no evidence in vivo that inhibitors of these enzymes significantly affect the metabolism of paliperidone; they contribute to only a small fraction of total body clearance. In vitro studies demonstrated that paliperidone is a substrate of P-glycoprotein (P-gp) (see Drugs Having No Clinically Important Interactions with INVEGA SUSTENNA under Interactions).
In vitro studies in human liver microsomes demonstrated that paliperidone does not substantially inhibit the metabolism of drugs metabolized by cytochrome P450 isozymes, including CYP1A2, CYP2A6, CYP2C8/9/10, CYP2D6, CYP2E1, CYP3A4, and CYP3A5. Therefore, paliperidone is not expected to inhibit clearance of drugs that are metabolized by these metabolic pathways in a clinically relevant manner. Paliperidone is also not expected to have enzyme inducing properties.
Paliperidone is a weak inhibitor of P-gp at high concentrations. No in vivo data are available, and the clinical relevance is unknown.
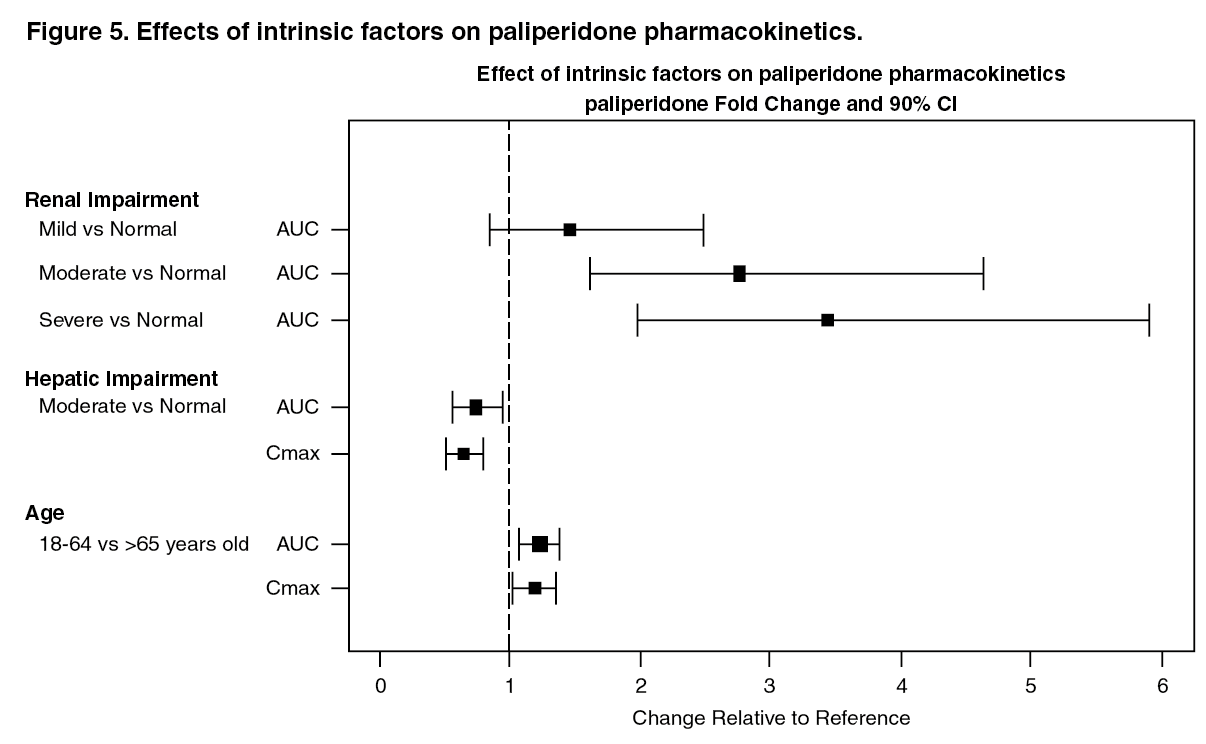
Studies in Specific Populations: No specific pharmacokinetic studies have been performed with INVEGA SUSTENNA in specific populations. All the information is obtained from studies with oral paliperidone or is based on the population pharmacokinetic modelling of oral paliperidone and INVEGA SUSTENNA. Exposures of paliperidone in specific populations (renal impairment, hepatic impairment and elderly) are summarized in Figure 5 (see Dosage Adjustments under Dosage & Administration and Use in Specific Populations: Renal Impairment under Precautions).
After oral administration of paliperidone in patients with moderate hepatic impairment, the plasma concentrations of free paliperidone were similar to those of healthy subjects, although total paliperidone exposure decreased because of a decrease in protein binding. Paliperidone has not been studied in patients with severe hepatic impairment (see Use in Specific Populations: Hepatic Impairment under Precautions).
After oral administration of paliperidone in elderly subjects, the Cmax and AUC increased 1.2 fold compared to young subjects. However, there may be age-related decreases in creatinine clearance (see Dosage Adjustments under Dosage & Administration and Use in Elderly under Precautions). (See Figure 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageBased on in vitro studies utilizing human liver enzymes, paliperidone is not a substrate for CYP1A2; smoking should, therefore, not have an effect on the pharmacokinetics of paliperidone.
Slower absorption was observed in females in a population pharmacokinetic analysis. At apparent steady-state with INVEGA SUSTENNA, the trough concentrations were similar between males and females.
Lower Cmax was observed in overweight and obese subjects. At apparent steady-state with INVEGA SUSTENNA, the trough concentrations were similar among normal, overweight, and obese subjects.
Toxicology: Nonclinical Toxicology: Carcinogenesis, Mutagenesis, Impairment of Fertility: Carcinogenesis: The carcinogenic potential of intramuscularly injected paliperidone palmitate was assessed in rats. There was an increase in mammary gland adenocarcinomas in female rats at 16, 47, and 94 mg/kg/month, which is 0.6, 2, and 4 times, respectively, the maximum recommended human dose (MRHD) of 150 mg of INVEGA SUSTENNA on a mg/m2 body surface area basis. A no-effect dose was not established. Male rats showed an increase in mammary gland adenomas, fibroadenomas, and carcinomas at 47 mg and 94 mg/kg/month. A carcinogenicity study in mice has not been conducted with paliperidone palmitate.
Carcinogenicity studies of risperidone, which is extensively converted to paliperidone in rats, mice, and humans, were conducted in Swiss albino mice and Wistar rats. Risperidone was administered in the diet for 18 months to mice and for 25 months to rats at daily doses of 0.63, 2.5, and 10 mg/kg, which are 0.2 to 3 times in mice and 0.4 to 6 times in rats the MRHD of 16 mg/day of risperidone on a mg/m2 basis. A maximum tolerated dose was not achieved in male mice. There were statistically significant increases in pituitary gland adenomas, endocrine pancreas adenomas, and mammary gland adenocarcinomas. The no-effect dose for these tumors was less than or equal to the MRHD of risperidone on a mg/m2 body surface area basis (see RISPERDAL package insert). An increase in mammary, pituitary, and endocrine pancreas neoplasms has been found in rodents after chronic administration of other antipsychotic drugs and is considered to be mediated by prolonged dopamine D2-receptor antagonism and hyperprolactinemia. The relevance of these tumor findings in rodents in terms of human risk is unknown (see Hyperprolactinemia under Precautions).
Mutagenesis: Paliperidone palmitate showed no genotoxic potential in the Ames reverse mutation test or the mouse lymphoma assay. No evidence of genotoxic potential for paliperidone was found in the Ames reverse mutation test, the mouse lymphoma assay, or the in vivo rat micronucleus test.
Impairment of Fertility: No fertility studies were conducted with paliperidone palmitate.
In a rat fertility study orally administered paliperidone increased pre- and post-implantation losses and slightly decreased the number of live embryos at doses up to 2.5 mg/kg/day, a dose which is 2 times the MRHD of 12 mg on mg/m2 basis. This dose also caused slight maternal toxicity but there was no effect on the percentage of treated female rats that became pregnant. Pre- and post-implantation losses, the number of live embryos and maternal toxicity were not affected at 0.63 mg/kg/day, a dose, which is half of the MRHD of 12 mg/day of orally administered paliperidone on mg/m2 basis. The fertility of male rats was not affected at oral doses of paliperidone of up to 2.5 mg/kg/day, which are up to 2 times the MRHD of 12 mg on mg/m2 basis, although sperm count and sperm viability studies were not conducted with paliperidone.
In a sub-chronic study in Beagle dogs with risperidone, which is extensively converted to paliperidone in dogs and humans, all doses tested 0.31 to 5.0 mg/kg/day, which are 0.6 to 10 times the MRHD of 16 mg on mg/m2 basis, resulted in decreases in serum testosterone and decreases in sperm motility and concentration. Serum testosterone and sperm parameters partially recovered, but remained decreased at the last observation two months after treatment was discontinued.